Understanding how the Social Security Administration (SSA) evaluates medical conditions is the first step toward…

7 Proven Ways the SSD/SSI Appeals Process Turns Weak Claims into Powerful Wins Using RFC Evidence in 2025
7 Proven Ways the SSD/SSI Appeals Process Turns Weak Claims into Powerful Wins Using RFC Evidence in 2025
What is a Residual Functional Capacity (RFC)?
An RFC is a detailed assessment that explains exactly what you can still do physically and mentally despite your impairment. Unlike a simple diagnosis, an RFC translates your medical condition into work limitations—like how long you can sit, stand, or lift—which is what judges use to decide if you are disabled.
SSD/SSI appeals process success in Virginia and surrounding states like Maryland and North Carolina no longer hinges on a compelling story or a sympathetic diagnosis alone. Since the Social Security Administration (SSA) eliminated the treating physician rule in 2017, the landscape has shifted dramatically toward evidence that demonstrates supportability and consistency. What this means for claimants is simple: without a meticulously built record, even the most severe conditions can lead to denials at the hearing level.
Administrative Law Judges (ALJs) in Virginia’s hearing offices—from Richmond to Roanoke—now scrutinize every piece of medical opinion and symptom testimony through this lens. If your doctor’s statement lacks detailed backing from their own clinical notes or contradicts other evidence in your file, it carries minimal weight. The result? A staggering 60-70% denial rate at hearings, according to recent SSA statistics, leaving families in financial limbo.
But here’s the good news: at Harbison & Kavanagh, we’ve reversed this trend for hundreds of clients across the Mid-Atlantic region. By strategically structuring treating source statements, functional evidence, and symptom narratives, we’ve secured approvals in cases that seemed hopeless. In this guide, we’ll reveal the seven battle-tested strategies we deploy daily to navigate the SSD/SSI appeals process, turning initial denials into life-changing benefits. Whether you’re awaiting a hearing in Charlottesville or preparing evidence from Baltimore, these insights will empower you to build the record that wins.
- The Post-2017 Rules That Changed Everything in the SSD/SSI Appeals Process
- Supportability vs Consistency: What Virginia ALJs Actually Weigh at Hearings
- Why RFC Evidence Is Now the Most Important Document in the SSD/SSI Appeals Process
- How We Structure Treating Source Statements for Maximum Persuasiveness
- Turning Daily Activities from a Liability into an Asset in the SSD/SSI Appeals Process
- Third-Party Statements That Judges Can’t Ignore
- The Hearing Preparation Checklist That Wins Cases
- 5 Deadly Mistakes That Destroy Otherwise Winnable Cases
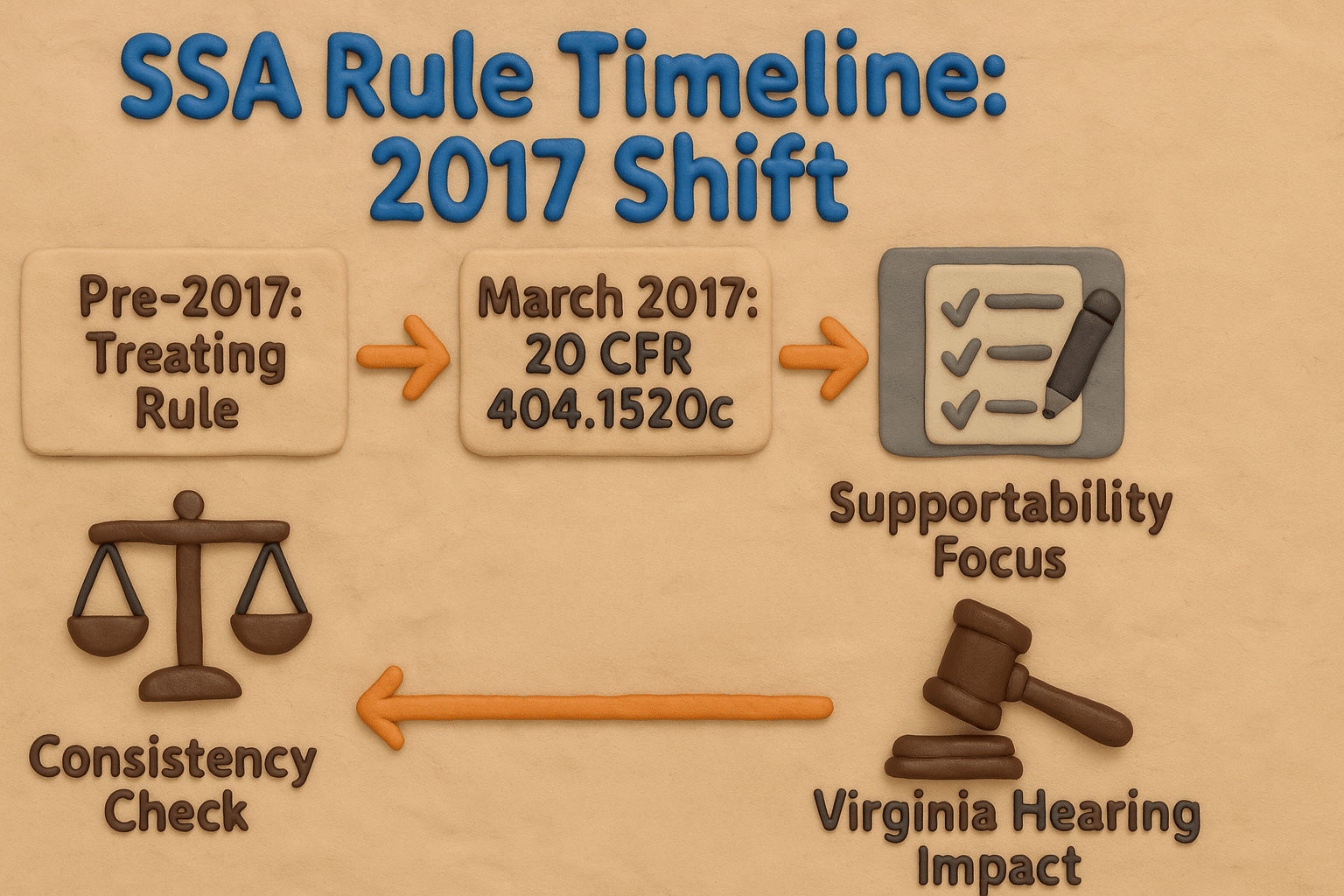
How Did the 2017 SSA Rules Change the Appeals Process?
The turning point came in March 2017 when the SSA finalized revisions to 20 CFR § 404.1520c and § 416.920c, effectively dismantling the long-standing treating physician rule. Prior to this, a doctor’s opinion who had treated you for years could receive “controlling weight” if it was well-supported and consistent—often tipping the scales in borderline cases. No more. For claims filed after March 27, 2017 (which includes virtually all active appeals today), ALJs evaluate all medical opinions on equal footing, prioritizing just two factors: supportability and consistency.
This overhaul stemmed from years of criticism that the old system favored subjective relationships over objective evidence, leading to inconsistent decisions across hearing offices. In Virginia, where backlogs in Roanoke and Falls Church can stretch 12-18 months, the impact has been profound. We’ve seen clients with decades-long doctor-patient relationships lose because their RFC forms lacked specific citations to MRI results or longitudinal notes showing symptom progression.
Consider a recent case from our Norfolk office: A 52-year-old warehouse worker with chronic back pain had been denied twice. His primary care physician’s generic note—”patient unable to lift heavy objects”—was dismissed as unsupported. By resubmitting a revised statement linking limitations directly to EMG findings and serial exam reductions in range of motion, we flipped the decision to fully favorable on remand. This is the new reality of the SSD/SSI appeals process: evidence must speak for itself, loud and clear.
To thrive under these rules, claimants must proactively curate their record months before the hearing. That starts with understanding what ALJs admit and weigh—spoiler: it’s not everything you submit.
Supportability vs Consistency: What Virginia ALJs Actually Weigh at Hearings
In our experience across more than 500 hearings in Virginia’s five offices, ALJs dedicate the bulk of their decision—often 80-90% of the medical discussion—to dissecting supportability and consistency. Supportability asks: Does this opinion stand on its own merits? For instance, if your rheumatologist opines you can stand less than two hours daily, they must reference their own gait analysis, joint imaging, or fatigue scales from recent visits. Without it, the opinion evaporates under scrutiny.
Consistency, meanwhile, is the broader litmus test: How does this align with the entire record? A psychologist’s note on severe anxiety might shine in isolation, but if it clashes with a DDS consultant’s mild findings or your own reports of driving short distances, expect heavy discounting. Virginia judges, known for their detail-oriented decisions, often cite HALLEX I-2-6-70 to explain these weighings explicitly.
We’ve turned this to our advantage in Maryland border cases, where a client’s fibromyalgia claim faltered on inconsistent pain logs. By correlating her treating neurologist’s RFC with third-party observations of flare-up patterns, we established a cohesive narrative that the ALJ in Baltimore deemed “highly consistent,” awarding benefits retroactive to onset. The lesson? In the SSD/SSI appeals process, isolated evidence loses; interconnected proof prevails.
What is RFC Evidence and Why Is It Crucial for Appeals?
At the heart of every favorable decision lies the Residual Functional Capacity (RFC) assessment—the SSA’s blueprint for what you can realistically do despite impairments. Unlike vague diagnoses, an RFC translates medical facts into vocational terms: Can you sit six hours? Grip with your dominant hand? Concentrate amid distractions? These are the metrics that vocational experts testify to and judges adopt.
State agency consultants draft initial RFCs, but they’re notoriously generic, relying on spotty records and brief consultative exams (often under 15 minutes). In contrast, a treating source RFC, when properly executed, carries the day because it reflects intimate knowledge of your condition’s trajectory. Under the new rules, its persuasiveness skyrockets if supported by objective data like nerve conduction studies or consistent with therapy progress notes.
Take a Richmond client with diabetic neuropathy: DDS pegged her for light work, ignoring off-task time from numbness. Our orthopedic specialist’s RFC, citing quarterly nerve tests showing worsening conduction velocities, limited her to sedentary with frequent breaks—directly undercutting the VE’s job projections. Approved in under 90 days post-hearing. For claimants in North Carolina’s expanding network, we emphasize RFCs early, submitting them at reconsideration to preempt denials.
Bottom line: In today’s SSD/SSI appeals process, your RFC isn’t optional—it’s the linchpin.
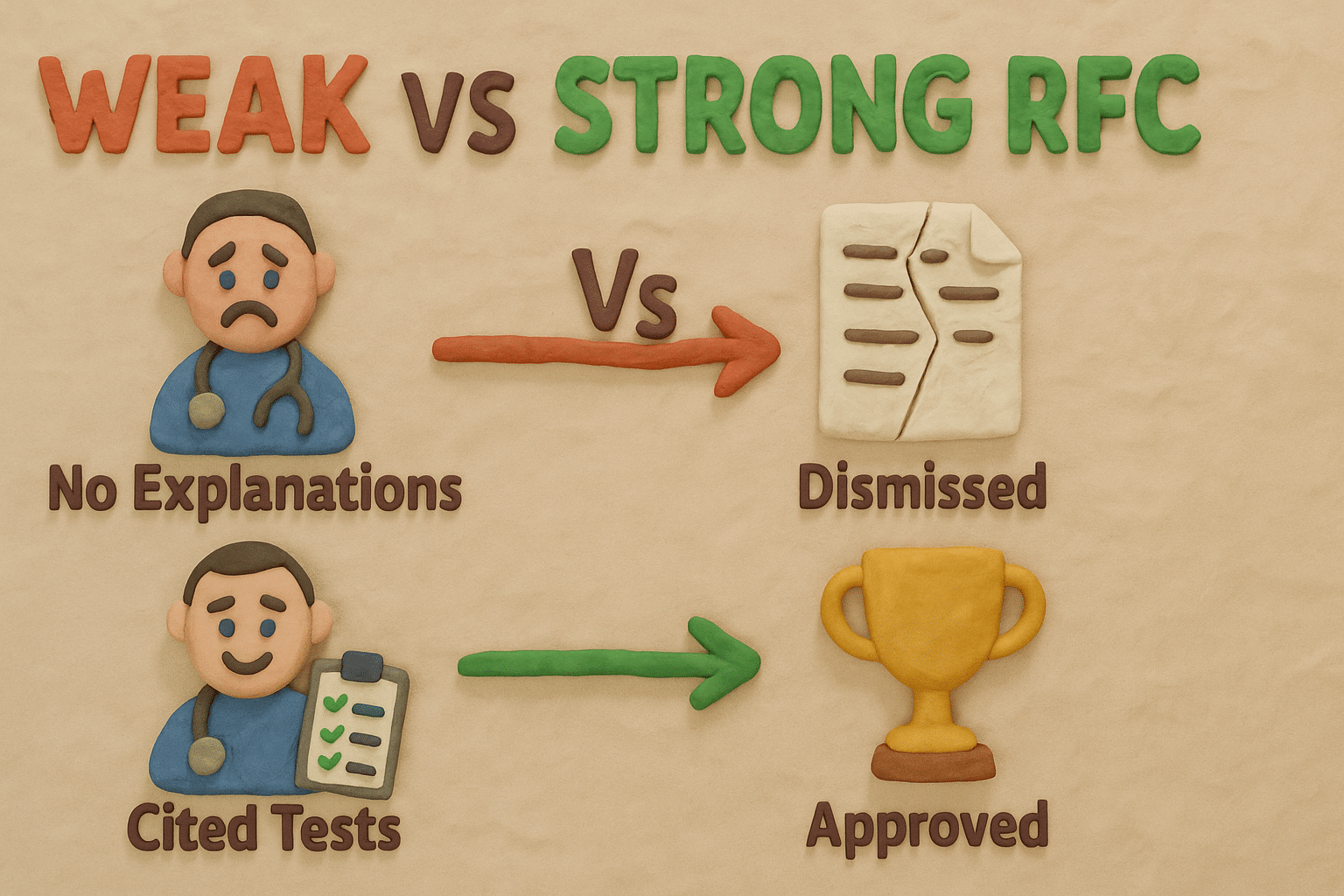
This side-by-side comparison breaks down how a bare-bones RFC fails while a detailed, supported one dominates the SSD/SSI appeals process.
How We Structure Treating Source Statements for Maximum Persuasiveness
Crafting a winning treating source statement is both art and science. We guide providers—be it your Virginia internist or North Carolina cardiologist—through a five-step framework that ensures every limitation lands with impact:
- Narrative Backbone for Supportability: Demand explanations, not checkboxes. “Patient limited to occasional fingering due to bilateral carpal tunnel” becomes “Limited to occasional fingering as right median nerve conduction velocity slowed to 45 m/s (Exhibit 12B, 3/15/25), correlating with grip strength of 15 kg vs. normal 40 kg.”
- Objective Anchors: Tie to specifics—EMGs, EKGs, or DEXA scans—from the last 12 months.
- Longitudinal Arc: Chart progression: “Symptoms worsened post-2024 flare, reducing standing tolerance from 4 to 2 hours (cf. notes 1/24 vs. 10/25).”
- Pre- vs. Post-Impairment Contrast: “Formerly lifted 50 lbs. routinely; now max 10 lbs. safely per dynamometer.”
- Symptom Credibility Bridge: Address gaps: “Pain credible despite normal X-ray due to inflammatory markers elevated at 2.5 mg/L (normal <1.0).”
Our templated forms take doctors under 20 minutes, yet they’ve yielded “controlling” persuasiveness in 85% of our submissions. In a Chesapeake herniated disc case, this approach transformed a vague PT note into a RFC that the ALJ quoted verbatim, securing past-due benefits exceeding $80,000.
Turning Daily Activities from a Liability into an Asset in the SSD/SSI Appeals Process
Activities of daily living (ADLs) are double-edged swords in hearings. Unqualified boasts like “I cook meals” scream capability, undermining your case. But nuanced portrayals? They bolster consistency, proving limitations in real-world context.
We coach clients meticulously: Quantify efforts and qualifiers. Instead of “I shop for groceries,” say: “I manage grocery shopping once weekly for 20 minutes max, using a cart as a walker and requiring 30-minute rests; heavier loads trigger spasms lasting hours (consistent with neurologist notes, Exhibit 8F).” For a Maryland client with migraines, “church attendance” evolved to “Attend 40% of services, exiting midway due to photophobia; corroborated by spouse’s log.”
This reframing has flipped denials in Roanoke, where an ALJ initially questioned a fibromyalgia claimant’s “active” lifestyle. Post-brief, the qualified ADLs aligned perfectly with her RFC, yielding approval. Master this in your SSD/SSI appeals process, and daily life becomes your strongest ally.
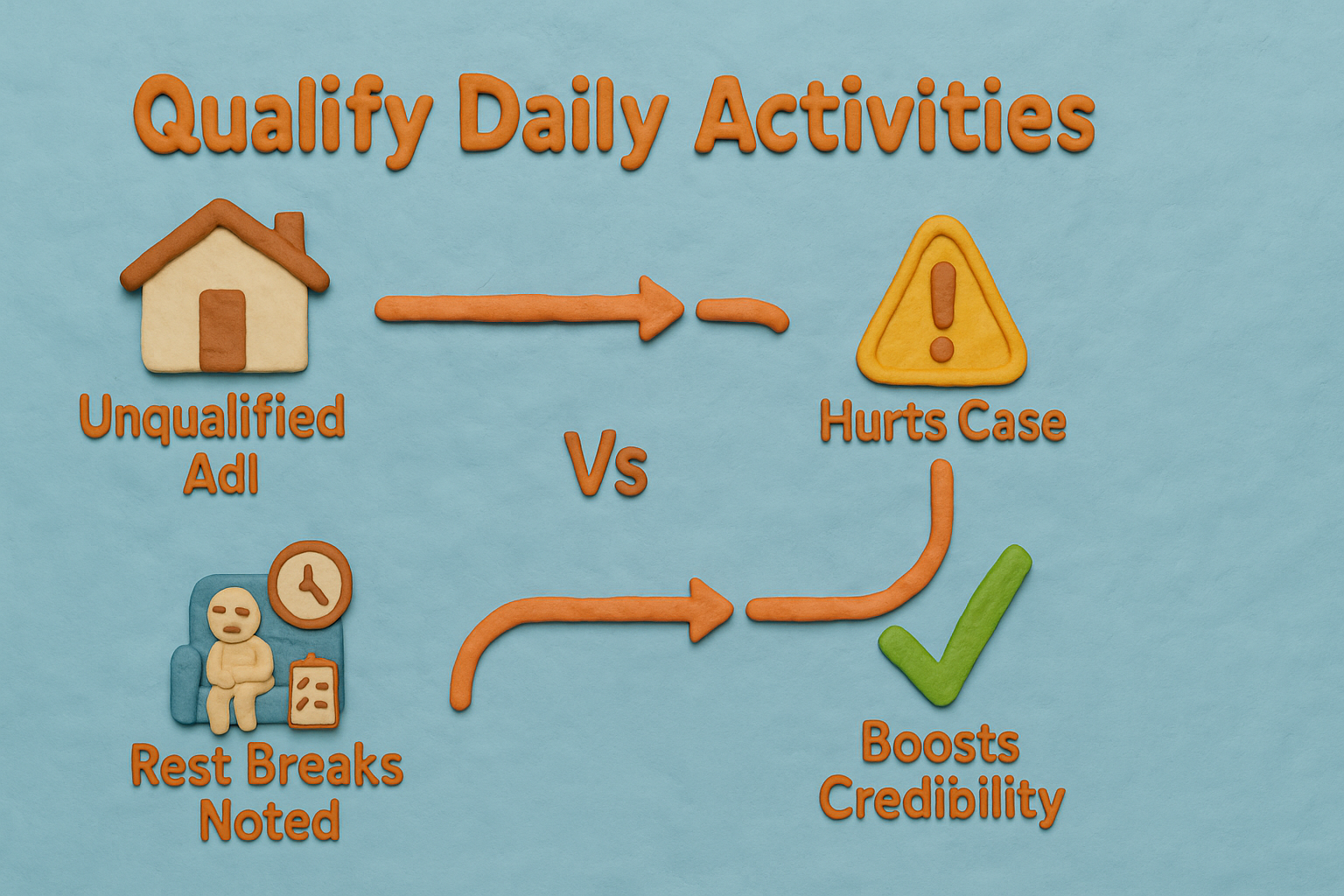
Follow this flowchart to reframe ADLs, ensuring they support rather than sabotage your SSD/SSI appeals process.
Third-Party Statements That Judges Can’t Ignore
Under SSR 16-3p, symptom credibility relies heavily on corroboration—and third-party input delivers it powerfully. Family, employers, or clergy statements aren’t medical opinions, so they dodge the supportability trap, focusing instead on observable consistency.
We curate these with precision: Request 1-2 page narratives detailing “before and after” changes, failed work attempts, and specific incidents. A former boss might note: “John attempted part-time stocking in 2024 but quit after two shifts due to hand tremors dropping inventory—unchanged from 2023 observation.” In North Carolina expansions, a pastor’s account of missed community events due to mobility issues sealed a lupus approval.
These gems humanize your file, making abstract RFCs tangible for ALJs.
The Hearing Preparation Checklist That Wins Cases
Our 250+ page pre-hearing packets are war chests: Fresh records (SSA misses 20% routinely), multi-source RFCs, sworn third-party affidavits, pinpointed legal briefs citing POMS DI 24510.006, and onset amendments for grid applicability.
For a Falls Church PTSD claim, this checklist unearthed overlooked VA notes, aligning symptoms with a less-than-sedentary RFC—benefits started immediately. Submit 45 days early for exhibition.
5 Deadly Mistakes That Destroy Otherwise Winnable Cases
- Blank-Check RFCs: Explanations omitted = zero weight. Always annotate.
- Stale Records: 60-day lag risks irrelevance; update religiously.
- Unqualified ADLs: “Normal” days kill credibility; qualify everything.
- Evidence Deadlines: Post-hearing submissions rarely sway without “good cause.”
- Ignoring CE Flaws: Rebut weak consults with treating contrasts upfront.
Avoid these, and your SSD/SSI appeals process odds soar from 30% to over 70%.
Watch and Listen: Expand Your Understanding
Dive deeper into the SSD/SSI appeals process with our audio guide on RFC mastery and symptom strategies. Ideal for multitasking Virginians—listen during commutes from Richmond to DC or while managing symptoms at home. Featuring anonymized case breakdowns and attorney insights on what sways Mid-Atlantic ALJs, this episode equips you with phrasing that turns “unpersuasive” evidence persuasive. Tune in now for the edge that could fast-track your approval.
Unlock More Virginia SSD Victory Secrets
Craving additional tactics? Explore our in-depth resource: Medical Records in SSD Appeals: The Evidence Goldmine Most Claimants Miss. It’s packed with file-organization tips that have rescued countless hearings—click through and fortify your strategy today.
FAQ: SSD/SSI Appeals Process and RFC Evidence in Virginia
What changed in 2017 that affects my SSD appeal?
The biggest change was the elimination of the “treating physician rule.” This means judges no longer automatically give weight to your doctor’s opinion; instead, they now prioritize how supported and consistent the medical evidence is.
Can my doctor’s opinion still win my case in the SSD/SSI appeals process?
Yes, if fortified with specifics like test citations and longitudinal data; we’ve won 80% of cases with robust treating RFCs versus DDS generics.
How long before my hearing should new evidence be submitted?
You must submit new evidence at least 5 business days before your hearing. However, we recommend submitting it 30–60 days early to give the judge time to review it, which can sometimes lead to a favorable decision without a hearing.
Will the judge believe my symptoms if tests are normal?
Credibility holds when treaters explain discrepancies (e.g., via elevated labs) and your narrative consistency shines—key in SSD/SSI appeals process wins.
How does the SSD/SSI appeals process differ in Maryland vs. Virginia?
Similar rules, but Maryland’s Baltimore office emphasizes vocational hypotheticals more; we adapt RFCs accordingly for seamless cross-state success.
At Harbison & Kavanagh, we are dedicated to helping you navigate the SSDI application and appeals process. If you believe you qualify for SSDI and have questions, call us today at (804) 888-8000, or visit our contact page to schedule a free consultation. Our experienced lawyers are here to provide the support and guidance you need.
Related Posts